Cancer Prevention Publicity Week | Chen Haiquan: Screening lung cancer, it is not necessary for non-high-risk groups to do CT once a year.

The World Health Organization has put forward that "one third of cancers can be completely prevented"-the so-called cancer prevention lies in "prevention". In China, lung cancer ranks first in terms of morbidity and mortality, so it is the top priority of prevention and control. On the occasion of the National Cancer Prevention and Control Publicity Week, China Cancer Foundation and the "medical community" hosted the "2020 Cancer Prevention and Control in Action" activity, and invited Professor Chen Haiquan from the Department of Thoracic Surgery of the Cancer Hospital affiliated to Fudan University to tell us about lung cancer screening and prevention and control.
We have summed up five key words of Professor Chen Haiquan about early lung cancer screening and treatment. Come and take notes ~
01
Keywords: 1. Popularization of low-dose CT
When the sun rises in the east and it rains in the west, LDCT becomes a sharp tool for early lung cancer screening.
The National Lung Cancer Screening Test (NLST) began in 2002. A total of 53,454 smokers aged 55-74 from 33 research sites in the United States were randomly assigned to the LDCT group and the X-ray chest film group for regular lung cancer screening. The results of 6.5 years’ follow-up show that the screening of low-dose spiral LDCT once a year for three years in high-risk groups can increase the detection rate of lung cancer by 13% and reduce the mortality rate by 20%. NLST research is of great significance in the field of lung cancer screening. Because of ending the long-term controversy about whether LDCT can reduce lung cancer mortality, the research ended ahead of schedule and was published in the New England Journal of Medicine.
Different from the West, the cost of low-dose CT screening in China can be said to be affordable for everyone. In the United States, it was not until 2014 that the government medical insurance covered the cost of low-dose CT screening, and at present it only covers people over 65, while people under 65 can only be covered by private insurance. However, in China, the situation of low-dose CT lung cancer screening is very different from that in the United States. The cost of low-dose CT screening in China is only 200 RMB, which can be said to be only the price of a steak in the United States.

The examination fee of low-dose CT in China is very low, and the radiation dose of low-dose CT is reduced by 75%~90% compared with conventional CT. At the same time, compared with X-ray chest film, it can find tiny lesions of several millimeters and tumors with tricky positions. Then, since low-dose CT screening has good screening advantages and economic popularity, which groups are suitable for lung cancer screening? In the United States, at present, the only high-risk population in NLST trial that proves that LDCT screening is effective is: the age is 55 -74 years old, with at least 30 packs/year of smoking history, and if you quit smoking, the smoking cessation time is less than 15 years. It is recommended to conduct low-dose CT screening for this group of people every year. And slightly different from the United States, China suggested that low-dose CT screening of high-risk groups should be more extensive, including:
Age ≥40 years old, and have any of the following risk factors:
1. Smoking ≥20 packs/year (or 400 packs/year), or smoking ≥20 packs/year (or 400 packs/year) and quitting smoking for < 15 years;
2 environmental or high-risk occupational exposure history (such as asbestos, beryllium, uranium, radon and other contacts);
3. Chronic obstructive pulmonary disease, diffuse pulmonary fibrosis or previous history of tuberculosis;
4. Those who have suffered from malignant tumors or have a family history of lung cancer.
02
Keyword 2: Pay attention to new high-risk groups
New high-risk groups have emerged: young people, non-smokers and women.
In 2013 -2014, the thoracic surgery team of Fudan University Cancer Hospital conducted a LDCT lung cancer screening study (FUSCC) on residents in Minhang, Shanghai, and found a special group of lung cancer-young, non-smoking women. This subverts people’s previous cognition of high-risk groups of lung cancer (old age, smoking, male). In order to confirm this situation, the research team once again conducted LDCT screening on 8,392 hospital employees from 6 hospitals in different regions of China.
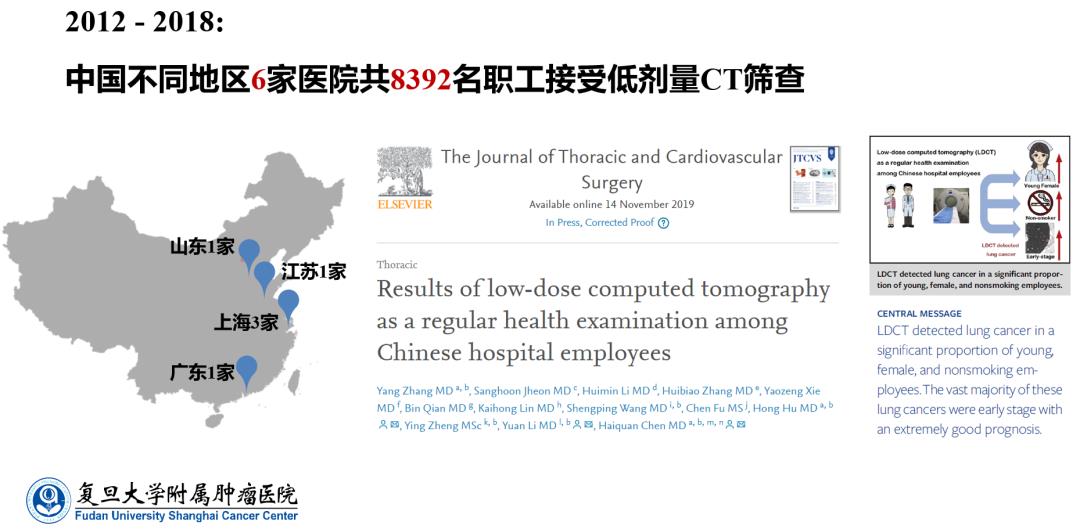
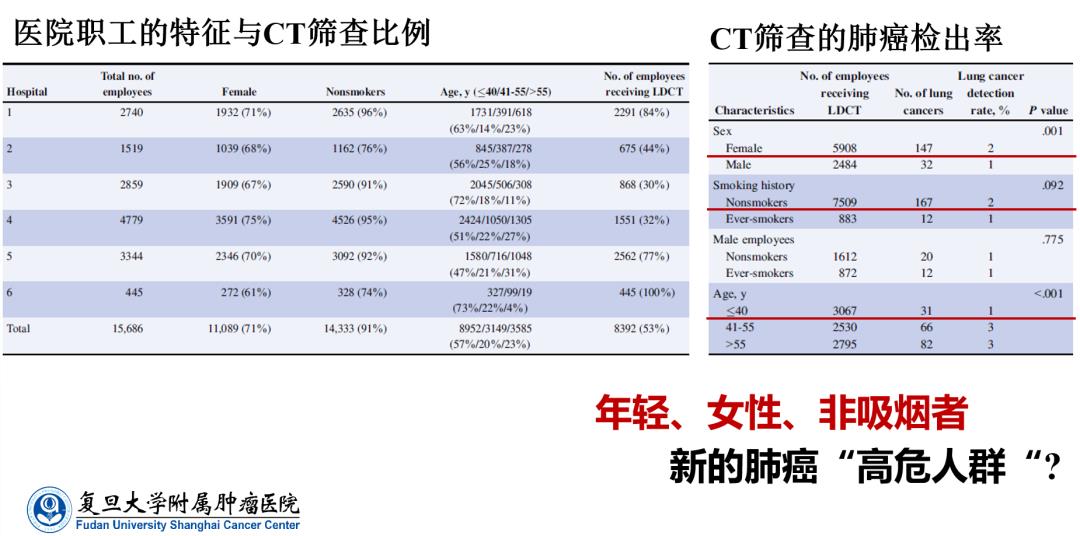
The results show that among 179 employees with lung cancer screened by CT, 147 are women, accounting for 82.1%, and only 32 are men. In terms of smoking habits, 167 people are non-smokers, accounting for 93.3%. The detection rate of women was 2.5%, which was significantly higher than that of men (1.3%). Among workers under 40 years old, the detection rate of lung cancer reached 1.0%. Therefore, this study once again pointed the high-risk group of lung cancer to young people, women and non-smokers.
Generally speaking, with the popularization of LDCT in China, the detection rate of early lung cancer has been greatly improved in the past 10 years. A phenomenon that cannot be ignored is that the incidence of lung cancer in China has increased significantly among young people, women and non-smokers. Therefore, this also poses two major challenges for our early lung cancer screening in the future:
1. Compared with the traditional definition of high-risk groups (old age, smoking, male), how to screen new high-risk groups such as "young, non-smoking, female"?
2. It is very important to study the etiology of young non-smoking female lung cancer population. How to further determine it in the future?
For more information on this topic, see: Do non-smoking women get more lung cancer? He pushed the "China issue" to the international level …
03
Keyword 3: Reasonable CT screening
The screening of early lung cancer is not covered by the whole population from young to old, but must distinguish between high-risk groups and low-risk groups. In view of the above-mentioned high-risk groups of lung cancer, it is recommended to conduct low-dose CT screening once a year; For low-risk people, CT screening can be accepted. If the result is negative, and if you keep a healthy lifestyle, you don’t need to check it every year. According to different age groups, you can choose to do CT screening every 3 years, 5 years and 10 years.
In addition, we also need to realize that CT can accumulate toxic dose, which will cause certain harm to human body. Because the screening methods of low-dose technology are harmful, according to the model of radiation hazard of atomic bomb explosion, it is estimated that in NLST screening test, one out of every 2,500 participants died of radiation. In addition, according to the current research data, in fact, most lung cancer patients are found in high-risk groups, such as smoking history, family history of cancer and so on. For non-high-risk groups, what we are emphasizing at present is to minimize unnecessary CT screening.
04
Keyword 4: GGO≠ Early lung cancer
Ground-glass nodules (GGO) are common in various lung diseases such as inflammation, edema, fibrosis and tumor. With the wide application of LDCT screening in clinic, we found that most of the lung cancers screened in China are asymptomatic, and most of them are GGO on CT. Therefore, it can be said that ground-glass nodular lung cancer has become the main target of lung surgery in China, but there is no conclusion on how to standardize the diagnosis and treatment of GGO.
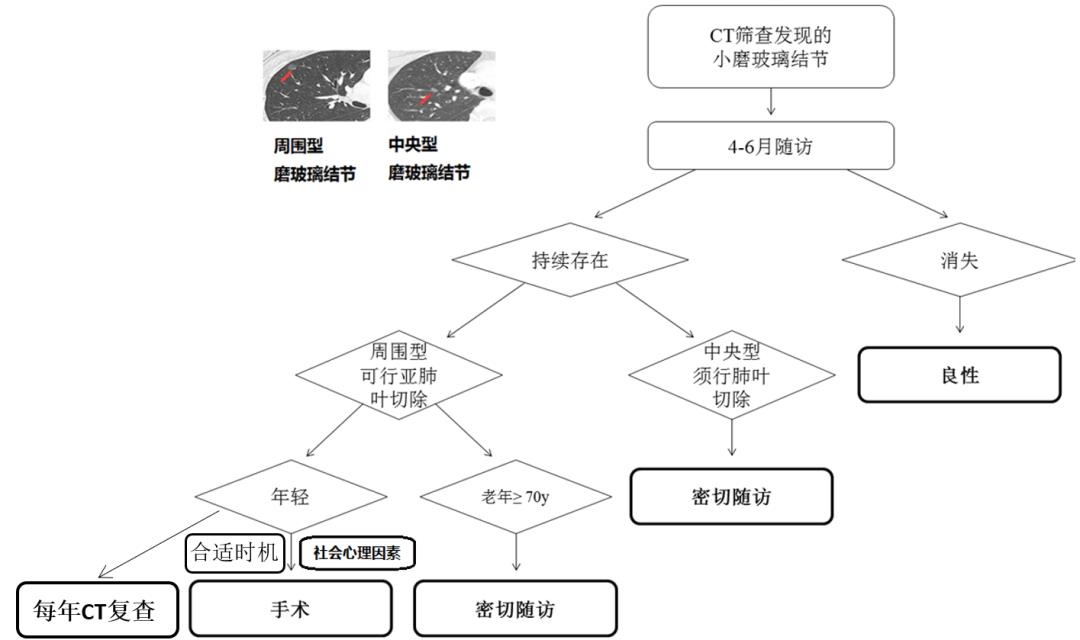
In the past, patients were worried and hoped for an early operation after being diagnosed with GGO, so as to avoid future troubles. But in fact, the diagnosis of "pure ground glass nodular lung cancer" should wait and see; If there is a growing trend of pure ground glass nodules, reconsider the operation. Therefore, for GGO, we should pay more attention to close follow-up. If the lesions become larger, the density becomes solid and the solid components increase during the review, this nodule may become cancerous, so it needs timely treatment.
Treatment process of pulmonary small GGO found by CT (Fudan standard)
05
Keyword 5: Avoid excessive diagnosis and treatment
In the process of early screening of lung cancer, LDCT can effectively improve the detection rate and reduce the mortality rate, but some studies show that 18.5% of lung cancer found by CT screening is overdiagnosed. Clinically, how to avoid "overdiagnosis" and "overtreatment" is also an important issue. The so-called overdiagnosis and overtreatment are nothing more than treating benign lesions as malignant tumors, treating early tumors as advanced tumors, and treating inert tumors as rapidly progressing tumors.
In order to avoid the "excessive" problem, the Department of Thoracic Surgery of Fudan University Cancer Hospital has established a standardized treatment process for follow-up and intervention of ground-glass pulmonary nodules. In recent 10 years, the benign rate of lung surgery is less than 10%. In addition, the research team also took the lead in proposing the innovative concept of "Minimally Invasive 3.0" in the world, and proposed for the first time to guide the surgical resection scope of lung adenocarcinoma through intraoperative frozen pathology. Under the guidance of intraoperative frozen pathology, the diagnostic accuracy of differentiating pre-invasive adenocarcinoma from invasive adenocarcinoma can reach 96.1%. For pre-invasive adenocarcinoma (in situ adenocarcinoma or micro-invasive adenocarcinoma), sub-lobectomy is enough, while for invasive adenocarcinoma, standard lobectomy plus systematic lymph node dissection is adopted.
For patients with atypical adenomatous hyperplasia/adenocarcinoma in situ/microinvasive adenocarcinoma, the 5-year recurrence-free survival rate of patients after lobectomy is 100%. The study was published in Journal of Clinical Oncology in 2016, which also means that early lung cancer surgery has taken an important step towards accurate and individualized treatment.
Wonderful view
1. What do you think are the main reasons for the abnormal increase in the incidence of lung cancer among non-smoking women? How to treat this phenomenon?
Professor Chen Haiquan:
Smoking is still a high-risk factor of lung cancer: in recent ten years, although we have found that the incidence of lung cancer in non-smoking women has increased, there may be high-risk factors other than smoking, such as second-hand smoke, kitchen fumes, air pollution, etc., but the cause can not be determined at present, and further research is still needed. The incidence of lung cancer in non-smokers is increasing, but it doesn’t mean that quitting smoking can’t prevent lung cancer. Smoking is still a high risk factor for lung cancer. Smoking lung cancer and non-smoking lung cancer are actually two diseases. For preventing lung cancer, quitting smoking is still an effective method.
2. How do we conduct standardized lung cancer screening? How much is once in a while?
Professor Chen Haiquan:
Emphasis on standardized screening of lung cancer: we divide the screening of lung cancer into high-risk and low-risk groups. Even though we say that low-dose spiral CT screening of lung cancer is economical and effective, it is not aimed at all the people. For people with high risk factors such as smoking, genetic history and environmental exposure, we suggest that low-dose CT screening can be carried out once a year; For non-high-risk people with healthy lifestyles, if you have to screen for lung cancer, you can consider reducing the frequency and it is completely unnecessary to do it every year.
3. What are the early symptoms of lung cancer? Can you detect it in your daily life?
Professor Chen Haiquan:
Early lung cancer generally has no obvious symptoms: in clinic, most lung cancer patients have clinical symptoms and then go to the hospital for treatment, which is late. Under normal circumstances, even if there is a mass with a diameter of 2 to 3 cm in the lung, we actually don’t notice any obvious influence from our physical condition. However, in ordinary life, we can pay more attention to it. If there is irritating dry cough and secondary infection, there may be expectoration. Phlegm and blood; Bright red or mixed with foam sputum and other symptoms; Or there are clubbed fingers (toes) or bone and joint hypertrophy, male breast development and other "extra-pulmonary symptoms", so we should be vigilant and go to the hospital for CT screening in time.
Doctor-patient question and answer
1. I am 36 years old. In August, 2018, my left upper lung apex was resected, and I was diagnosed as a tiny invasive adenocarcinoma. At an early stage, the doctor said that I didn’t need chemotherapy or medicine. Here I would like to consult Professor Chen and give some advice on regular check-up, diet and exercise direction. Is it necessary to do genetic testing? At ordinary times, my lungs still feel a little swollen. (Do 3 to 4 CT reexaminations every year. Is exercise suitable for doing push-ups? )
Professor Chen Haiquan:
If the pathological result is micro-invasive adenocarcinoma, no adjuvant treatment is needed after operation. Such patients should be normal people’s work and life after operation. With regard to postoperative reexamination, 3-4 CT reexaminations per year are definitely too many. Although there is no guideline for the frequency of postoperative reexamination, many of our studies and foreign studies show that the recurrence rate of such patients is 100% in 5 years, so we suggest that CT reexamination should be done within half a year after operation. If all patients are normal and under 50 years old, they can be reexamined every 3-5 years.
2. Thin layers 23.52.81, 7*5 in both lungs, and two small glass nodules 52.55, 4 mm in the right lung. Do you want to deal with them? The local doctor told me to follow up after half a year, because I had left upper lobe resection two years ago, and this situation occurred in the follow-up visit this year. What should Professor Chen do?
Professor Chen Haiquan:
If the physical examination ct finds 4mm ground glass nodules, there will be no problem after one year.
3. In stage 1B of lung adenocarcinoma, 50% were papillae, 40% were acinus, 5% were microemulsion and 5% were solid. Involve pleura. EGFR19 mutation. Is it necessary to target prevention after chemotherapy?
Professor Chen Haiquan:
If it is stage IB lung cancer, the necessity of postoperative chemotherapy needs further study. Since it has been done, subsequent targeted therapy should be unnecessary.
Expert introduction

Professor Chen Haiquan
Chen Haiquan: Doctor of Medicine, chief physician, professor and doctoral supervisor. Director, Institute of Chest Tumor, Fudan University; Director, Department of Thoracic Surgery, Cancer Hospital Affiliated to Fudan University; Chief Expert, Multidisciplinary Diagnosis and Treatment Group of Chest Tumor; Director, Lung Cancer Prevention and Treatment Center. Former president of Shanghai Chest Hospital. Member of the American College of Thoracic Surgery (AATS) and member of the membership development committee (2016-2017). Member of Board of Education (2019-) International Director of American Association of Thoracic Surgeons (STS) (2016-2019), Member of European Association of Thoracic Surgeons (ESTS) and Director of Asian Association of Thoracic Cardiovascular Surgery (ASCVTS) (2016-). Vice president of thoracic surgeon branch of Chinese Medical Association, member of Standing Committee of Lung Cancer Committee of China Anti-Cancer Association, member of thoracic and cardiovascular surgery society of Chinese Medical Association, vice chairman of thoracic surgery branch of Shanghai Medical Association, and chairman of thoracic tumor committee of Shanghai Anti-Cancer Association. Editorial Board of J THORAC CARDIOV SUR, Deputy Editor-in-Chief of J CANCER RES CLIN, Editorial Board of Am J Transl Res and J Thorac Dis. He presided over two key projects of the National Natural Science Foundation, general projects, municipal and ministerial key scientific research projects, etc.
Internationally, we innovatively put forward "Minimally Invasive Lung Cancer 3.0", "Sublobar Resection Guided by Frozen Pathology" and "Selective Lymph Node Dissection in Lung Cancer Surgery". From 2013 to 2018, he was invited to give lectures at the American Society of Thoracic Surgery (AATS) every year. In 2016, he served as co-chairman of the 96th annual meeting of the American Society of Thoracic Surgery, and chairman of AATS Focus on Thoracic Surgery: China. In 2017, he served as the vice chairman of the joint meeting of the 9th Asian Thoracic Surgery Club (ATSC) and Korean Thoracic Surgery Oncology Association (KATSO). Since 2008, he has been invited to give lectures at the University of Pittsburgh Medical Center, Massachusetts General Hospital of Harvard University, Kettering Cancer Center in Si Long (MSKCC), Vanderbilt University Medical Center, Zurich University Medical Center, and Leuven University Medical Center. Since 2017, he has been invited to write four editorials for JTCVS. Schuster distinguished lecture ship, Brian Hospital, Harvard University, 2020. As a correspondent or the first author, he has published more than 170 papers in SCI journals such as Cancer Cell, JCO, ANN SURG, JTO, NC, CCR, Cancer, JTCVS, ANN THORAC SURG, etc.By the end of 2019, the innovative achievements of 16 papers and 20 sub-papers have been included in 10 international guidelines for diagnosis, treatment and molecular detection of lung cancer, such as ASCO, ESMO, IASLC and ACCP. Two papers were collected by UpToDate, an internationally renowned evidence-based medicine database.

Author: Huanhuan
Editor: Xu Jia